Science Saved It, Execution Proved It: Schizophrenia's First New Mechanism in 70 Years
How a time-constrained 6-month proof-of-concept study and disciplined trial methodology transformed a shelved compound into a $14 billion breakthrough
In the past, we’ve had the privilege of speaking with two leaders whose work, separated by years and roles, converged to create one of the most significant advances in schizophrenia treatment in seven decades. Their stories (first from Dr. Anantha Shekhar’s scientific rescue at Indiana University, then Dr. Steve Brannan’s operational execution at Karuna Therapeutics) offers complementary lessons about what it takes to transform a promising mechanism into an approved therapy.
At Power, we work with sponsors to identify and recruit patients for neuropsychiatry trials… and these conversations revealed how foundational patient recruitment infrastructure is to trial success, from proof-of-concept through registration.
The group homes started calling within the first week. “Whatever you put this person on, please keep them on it,” they told Dr. Shekhar. “They are doing so well.”
This wasn’t expected. The compound, xanomeline, had been shelved by Eli Lilly after Alzheimer’s trials showed a 50% discontinuation rate. The company had moved on.
But Shekhar, John and Gertrude Petersen Dean of the School of Medicine at the University of Pittsburgh, saw potential others had overlooked. When Lilly prepared to discontinue xanomeline’s development, Shekhar had six months to prove it could work in schizophrenia. “We had six months literally to...get the drug out of Lilly and we had no money. We had to raise a couple hundred thousand,” he recalls.
His clinical research unit was already running other antipsychotic trials. The existing patient recruitment infrastructure let him move quickly. “Fortunately, I had a clinical research unit where I was doing other clinical trials...so we were able to quickly do a 20 patient study within six months.”
That small study (10 patients on xanomeline, 10 on placebo) showed encouraging results. Patients who typically needed weeks of hospitalization were going home in 5-6 days. The proof of concept was established.
But proving a concept and executing a registration program are different challenges. This is where the story shifts from scientific validation to operational discipline… and where patient recruitment strategy becomes foundational to trial success. At Power, we focus on systematic patient identification for neuropsychiatry trials, and the infrastructure that enables consistent site performance proved central to Karuna’s eventual success.
When Execution Becomes Everything
Dr. Steve Brannan joined Karuna Therapeutics in 2017 as employee number two. Karuna had licensed xanomeline in 2012 and combined it with trospium to mitigate peripheral side effects while preserving central efficacy.
At this stage, the question wasn’t whether the mechanism worked. It was whether they could run trials precise enough to demonstrate it.
What followed demonstrated clinical operations discipline. Brannan brought decades of experience from Eli Lilly, Novartis, Takeda, and Forum Pharmaceuticals. Critically, he worked with Sharon Sachs, who had extensive experience at GSK, as a clinical operations consultant.
“We just didn’t make the same mistakes,” Brannan notes. “We avoided pretty much everything.”
Mistake 1: Expanding Beyond Quality Sites
“There’s probably a limited number of really high quality sites doing this kind of work in the US,” Brannan explains. “You go past the A sites into the B sites and then the C sites. You just add more variance.”
Karuna kept their site list focused. “The sites working for us aren’t doing it because they know Karuna. They’re doing it because they know me and Sharon.”
This connects directly to patient recruitment strategy. When you maintain relationships with established sites, you can be selective with patient enrollment. When sites struggle to hit targets, compromises become more likely. See: The 6-Month Recruitment Misconception: Why Late Starts Impact Trial Success.
Shekhar emphasized similar discipline: “Very rigorously control the assessment of patients, very rigorously control the type of patients we were enrolling and the fidelity to the protocol across all of the sites. If you don’t do that, there’s so much noise and so much variability that you could lose the therapeutic signal.”
Mistake 2: Speed Without Discipline
Brannan’s example: at Takeda, the first wave of antidepressant trials went 0-for-8. Same compound, second wave went 4-for-5 positive. “One of the things was not getting in a hurry and doing stupid stuff.”
Six months after committing not to rush, leadership from both Lundbeck and Takeda was pushing for acceleration. “They can’t help themselves,” he says. “You need somebody that has the courage to sort of say no.”
Mistake 3: Ignoring the Data Stream
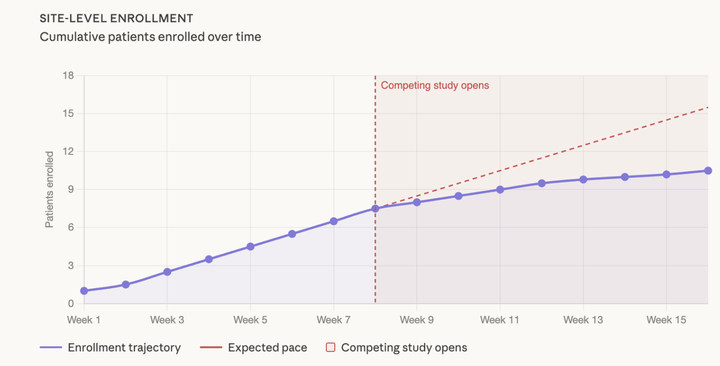
When one site enrolled three consecutive patients over age 55 (above the trial’s median of 42-44) Brannan called the PI directly. “How long is the geriatric convention in town?” The PI understood. He was funneling younger patients to a competitor’s trial. “The next three patients they did were all under the age of 55.”
The Protocol Simplicity Principle
Both leaders emphasized keeping trials focused. “The key question is: is the drug better than placebo,” Shekhar explains. “A lot of times people will say, ‘Why don’t we enrich our patients for X? Why don’t we try to discover a biomarker while we’re at it?’ What happens is that the study becomes very overburdened with questions.”
Brannan’s advice on advisory boards? “Use them for understanding science. If you have a proof of concept, make it simple. The use of that approach for answering the simple first question can sort of mess it up rather than help.”
Where It All Comes Together
Three years from Brannan joining to positive Phase 2 results. Continued success through Phase 3. FDA approval September 26, 2024. Bristol Myers Squibb acquired Karuna for $14 billion.
“It feels amazing,” Shekhar reflects. “This is why I went to medicine 40 years ago. And the first ever new treatment for that disease in 75 years is coming out of the work I did.”
For clinical operations teams, the approach is instructive: methodological discipline matters. Site quality over quantity. Optimal pacing over speed. Continuous monitoring over assumptions.
And critically: proactive patient recruitment infrastructure over reactive crisis management.
Both Shekhar and Brannan built on existing operational infrastructure. Shekhar’s unit was already running antipsychotic trials… the patient screening processes and site relationships made a six-month enrollment achievable. Brannan’s selective site strategy worked because he partnered only with investigators who had demonstrated patient access and enrollment capability.
As Brannan puts it: “I need the right patients at the right sites. Sounds simple, but it’s a lot harder.” For most sponsors, this challenge requires going beyond site databases… actively identifying and connecting with patients seeking trials. This is precisely what systematic patient identification enables: the ability to be selective, to maintain protocol fidelity, and to keep enrollment on pace without compromising on quality.
That discipline, applied to both trial design and patient recruitment strategy, transformed a previously shelved compound into the first new mechanism for schizophrenia in seven decades. The science was compelling. Execution made it possible. And execution required patients at the right sites, at the right pace, throughout the trial.
Power provides systematic access to patients actively seeking neuropsychiatry trials—delivering the qualified patient flow that execution discipline requires. Because perfect trial methodology without qualified patient flow still misses timelines. Let’s discuss your enrollment strategy.
Comments ()