The 6-Month Recruitment Misconception: Why Late Starts Impact Trial Success
Why waiting until "6 months left" dramatically increases your risk of missing enrollment deadlines
We know enrollment timelines are top of mind for many clin ops teams right now. If you're looking at your current trajectory and thinking "We've got 6 months left for enrollment," you're not alone... and there may be strategic opportunities to optimize your approach through early recruitment firm partnerships.
I've observed this pattern across numerous trials. Study teams progress confidently through site selection and activation phases. Then reality becomes apparent, based on the current trajectory the study is tracking 2 months behind. "We're behind schedule. We need to implement recruitment strategies immediately."
What follows are predictable operational challenges... and a steep learning curve in recruitment mathematics.
Here's why the "6 months left" approach often leads to timeline extensions... and what experienced clin ops teams do differently.
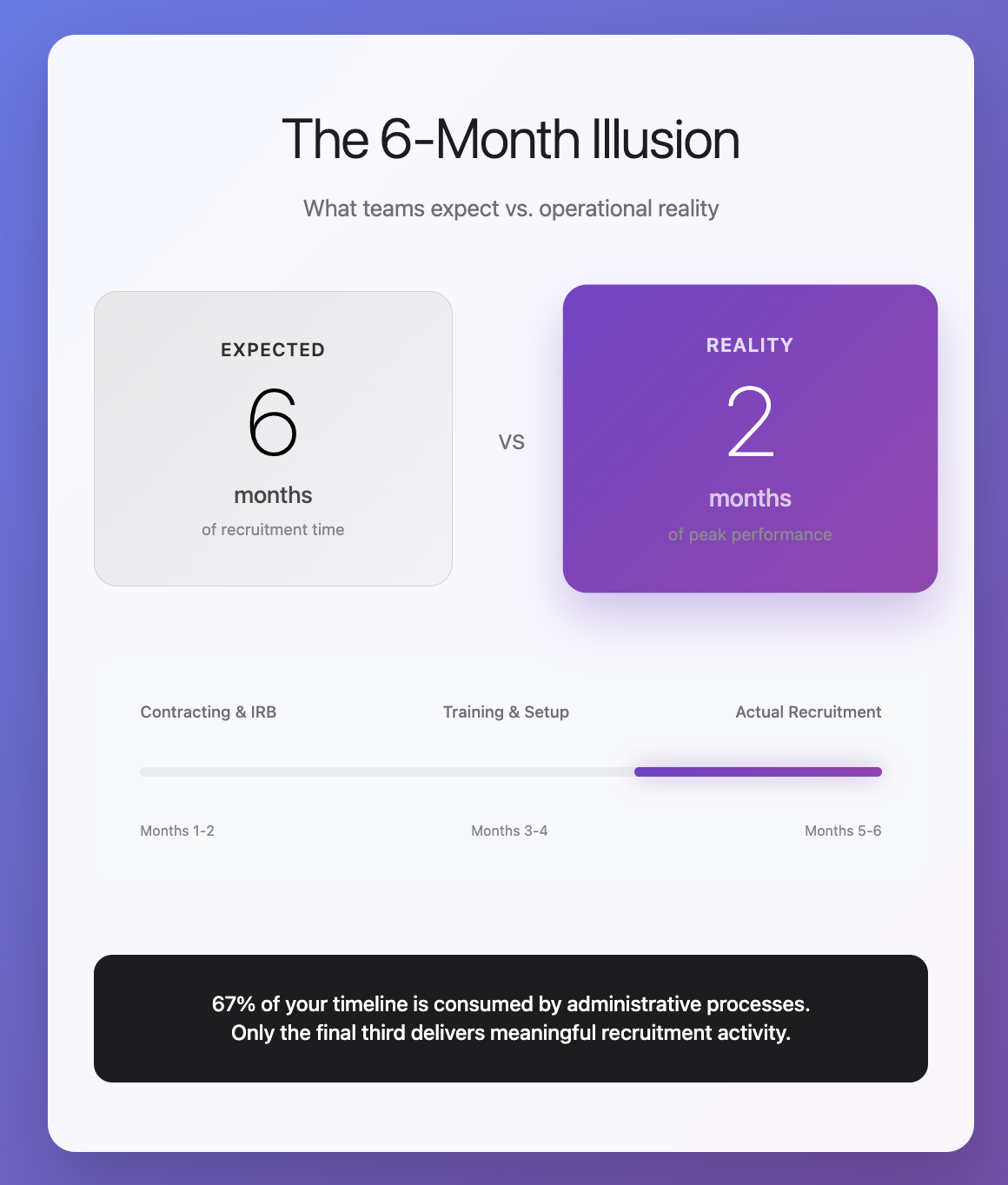
The Administrative Reality of “Late-Start” Recruitment
When you decide to implement external recruitment with (as a typical example) 6 months remaining, here's your actual operational timeline:
Months 1-2: Vendor contracting (4-6 weeks) and IRB amendment processes (6-8 weeks for complex studies, often running in parallel)
Months 3-4: Site onboarding and training, system integration, and recruitment material finalization
Months 5-6: Initial patient referral flow, site capacity assessment, and pipeline optimization
You, for example, anticipated 6 months of recruitment activity. In practice, you have 8-12 weeks of peak recruitment performance.
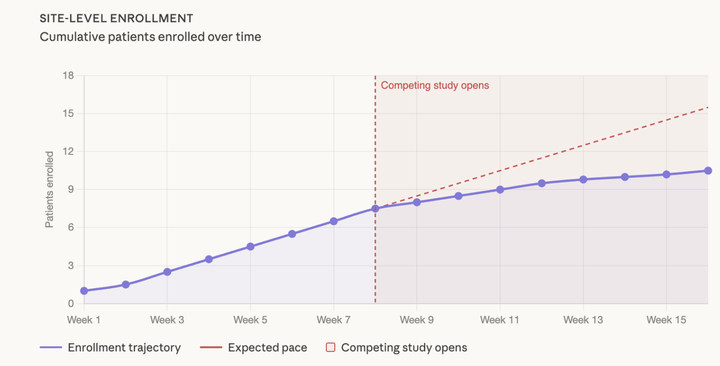
Meanwhile, many of your sites are experiencing their own enrollment challenges. As documented in previous analyses, most sites exhaust their readily available patient populations by (as a common example) month 6 and require systematic patient identification strategies to maintain consistent performance.
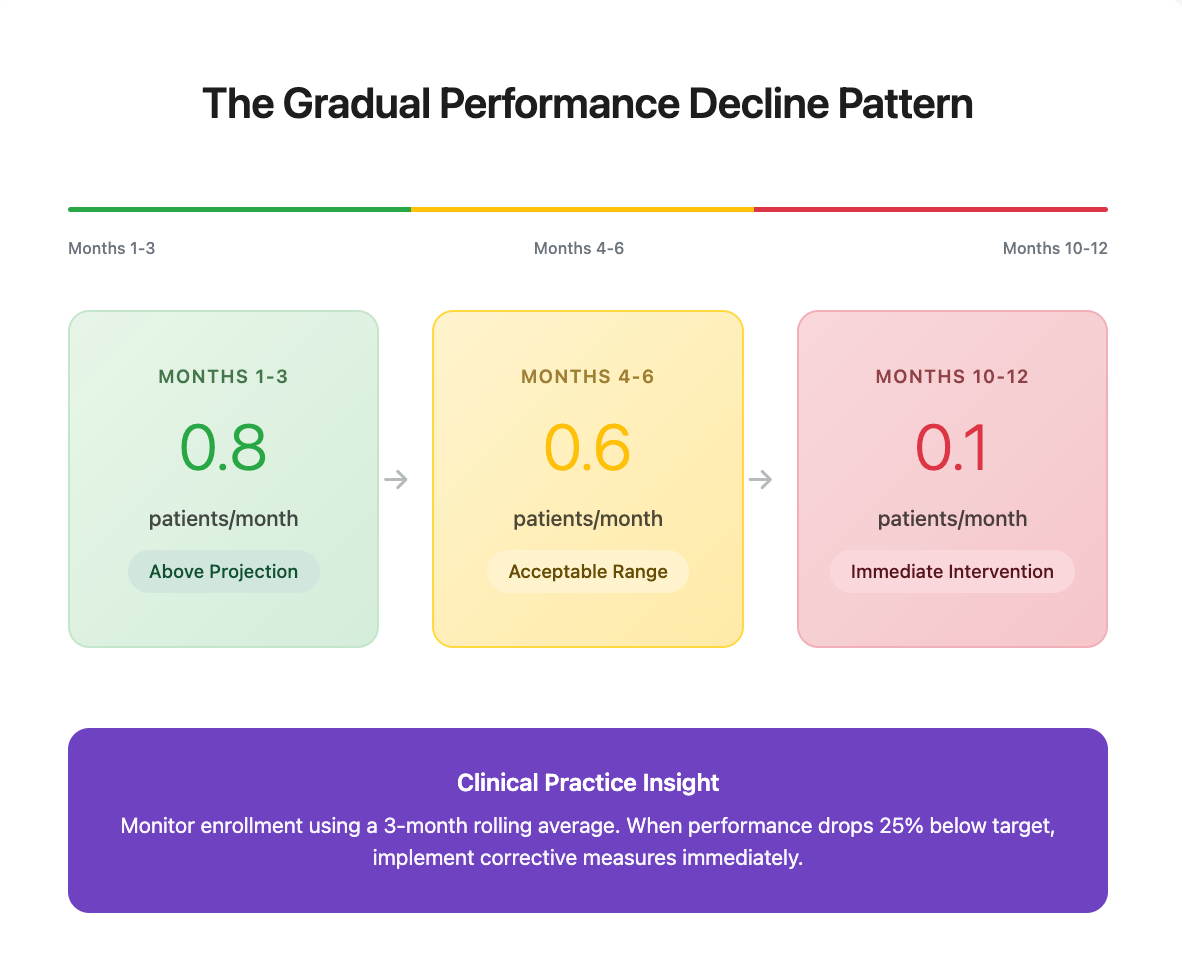
The Gradual Performance Decline Pattern
Most teams encounter this situation because early enrollment metrics appear acceptable:
Months 1-3: Sites enroll 0.8 patients/month (above projection)
Months 4-6: Maintaining 0.6 patients/month (slightly below target, but within acceptable range)
Months 10-12: 0.1 patients/month (requires immediate intervention)
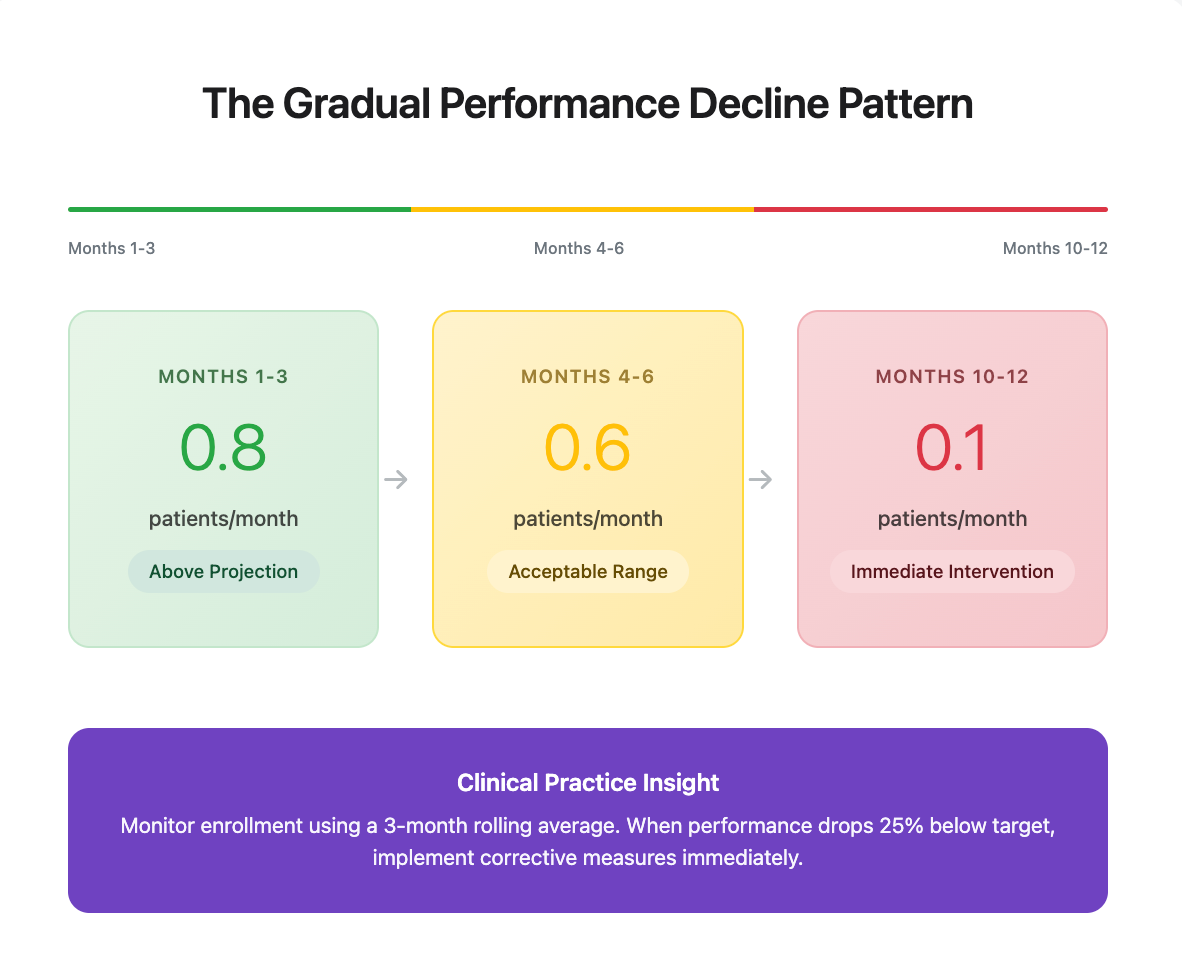
This pattern occurs consistently across therapeutic areas. Teams often don't recognize the gradual decline until enrollment becomes insufficient (and help is often needed).
Clinical Practice Insight: Monitor enrollment using a 3-month rolling average rather than monthly snapshots. When performance drops 25% below target, implement corrective measures immediately. On a related note, this is why we recommend managing patients in a “flow”, or rather, in time cohorts.
The Financial Impact of Delayed Implementation
A 4-month timeline extension typically results in $6M+ in direct operational costs, plus $24M+ in NPV impact from delayed market entry... representing over $30M in potential program value impact.
Reference our ROI analysis framework to calculate how these metrics apply to your specific program parameters.
The 12-Month Recruitment Performance Framework
Most successful trials require 12+ months of sustained recruitment performance to achieve aggressive enrollment targets.
The clinical rationale is clear. Sites maintain higher performance levels with systematic patient identification support, continuous referral flow prevents the typical month 6 “enrollment plateau,” and extended timelines allow for optimization and protocol adjustments.
The mathematics support this approach: Enrolling 150 patients over 12 months with consistent site support versus attempting to recover enrollment with 30 patients over 2 months. Without external recruitment infrastructure, most sites average 0.4 patients/month after month 6.
Evidence-Based Recruitment Planning
Successful clinical programs don't treat recruitment as a contingency plan. They integrate it as core trial infrastructure:
Initiate During Pre-Feasibility: Include recruitment planning during protocol development and site assessment phases. Budget recruitment infrastructure in initial financial models rather than as post-hoc additions.
Implement 3-4 Months Before FPFV: Begin recruitment vendor selection and contracting 3-4 months before First Patient First Visit (FPFV). This allows adequate time for IRB processes, site training, and system integration.
Maintain Sustained Performance: Plan for 12+ months of recruitment support (or whatever timeline best fits your trial) to ensure consistent site performance throughout the enrollment period.
Operational Mindset Adjustment
Traditional approach: "Let's assess site performance, then consider recruitment options if needed"
Evidence-based approach: "Let's ensure consistent site performance through systematic patient identification from trial initiation"
Old question: "When should we start recruitment?"
Better question: "How do we maintain 12 months of optimal enrollment performance?"
Implementation Recommendations
For trials in planning phase:
- Incorporate 12+ months of recruitment support in timeline projections
- Begin vendor evaluation during pre-feasibility and protocol finalization phases
- Establish performance monitoring: when 3-month rolling enrollment drops 25% below target, implement corrective measures immediately
For trials currently behind target:
- Calculate realistic recruitment timeline using the 60-day pipeline framework
- Prioritize recruitment investment... every month of delay significantly impacts program economics
- Focus on optimizing existing site performance with enhanced patient flow rather than solely expanding site networks
Clinical Operations Perspective
Every clinical program begins with optimistic site performance projections. The distinction between successful and delayed programs isn't superior forecasting ability... it's implementing systematic patient identification infrastructure from trial initiation rather than as a reactive measure.
Programs that consistently meet enrollment timelines typically aren't better at predicting site performance; they tend to be more effective at ensuring consistent site performance through early recruitment firm partnerships rather than reactive engagements.
Engage recruitment firms early. Maintain long-term partnerships. Avoid the 6-month misconception.
Have recruitment timing challenges you'd like us to address? Reply (brandon@witbhpower.com) with your specific operational questions for potential feature in future analyses.
Comments ()