The Alzheimer's Hypothesis Big Pharma Missed
Why a former Genentech director bet on cortisol over amyloid, and what pilot data showing 5x better efficacy could mean for patients
The Alzheimer’s Hypothesis Big Pharma Missed
After three decades developing drugs at Genentech and Principia, Steven Gourlay has seen enough failed Alzheimer’s trials to know the difference between real signal and noise. When he joined Actinogen four years ago, the Australian biotech had a negative Phase 2 trial and a molecule most would have written off. Today, he’s running what might be the most compelling alternative to amyloid antibodies—with pilot data in biomarker-positive patients suggesting substantially larger effects than approved drugs, delivered as a once-daily pill.
“I joke with some of the folks here that I haven’t missed a clinical trial for more than a decade and I’m not planning to start now,” Gourlay tells me. His track record backs it up: at Principia, he led multiple molecules through Phase 3, culminating in Sanofi’s acquisition for several billion dollars.
What attracted him wasn’t just the science—though decades of research links elevated brain cortisol to Alzheimer’s and depression—it was that nobody had ever successfully targeted it before. “It’s probably the best looking small molecule I’ve ever seen in my 35 years of drug development experience,” he says. Xanamem (emestedastat) selectively lowers cortisol in brain tissue while leaving the body’s normal stress response intact—something previous attempts couldn’t achieve.
The biology is straightforward once he explains it: “If you put a pellet of cortisol into a mammalian brain, you will see tissue dieback, neuronal dieback, around that pellet. Cortisol itself, certainly in high concentrations, is directly toxic to neurons.” Long-term steroid use causes depression, foggy thinking, and memory problems. Lower brain cortisol, protect neurons. Simple concept. Hard execution.
The Depression Trial That Proved It Works
Last year, their Phase 2a trial in 167 patients with major depressive disorder and cognitive impairment delivered statistically significant improvements over just six weeks. This was the first real evidence that controlling cortisol produces meaningful clinical effects. “This trial shows that Xanamem’s mechanism of cortisol control in the brain has major clinical impact,” Gourlay says.
But here’s where his experience shows. Cognitive assessments showed large improvements in both drug and placebo groups. “There was a very big placebo effect in cognition,” he explains. “When patients’ depression got better, their cognition improved independent of our drug.” Most companies would have spun that as a win. Gourlay saw it as noise requiring better trial design for Alzheimer’s. The depression benefit was real. The cognitive signal needed cleaner data.
Five Times Better Than Current Drugs?
The Alzheimer’s story gets more interesting. When Actinogen went back to their original negative trial and analyzed stored blood samples with modern biomarker tests, they found something striking. In patients with elevated pTau181 markers showing active disease, the treatment effect was massive—even over just 12 weeks.
Gourlay’s comparison to approved drugs is blunt: “The clinical benefit of these antibodies over 18 months is half a point on this 18-point scale. One point on the CDR-SB is regarded as the minimum clinically significant difference. So it’s been approved on half the clinically significant difference.”
His prediction: “We know there’s a lot of interest both from doctors and patients in a much more convenient option for Alzheimer’s. If we are indeed, as the pilot data suggests, five times better than these antibodies, I don’t think anybody’s going to take the antibody.”
The math matters here. Current approved drugs require infusion center visits every two weeks, cause brain swelling in some patients, and deliver effects most researchers consider below clinically meaningful thresholds. Actinogen’s pilot data in biomarker-positive patients suggests substantially larger effects from a once-daily pill with clean safety in more than 400 people treated across multiple trials.
Why Most Alzheimer’s Trials Fail
On the fatal mistake: “A number of companies have boasted about open-label data showing that the drug must be working because cognition didn’t get worse. But all of them that I know of, when they’ve actually done a placebo-controlled trial, didn’t work and they were misled by not having a placebo control.”
His approach: “I do follow a fairly strict scientific method when it comes to clinical trials. I do think clinical research should be as disciplined as any laboratory research.” The details matter—same raters across visits, standardized testing conditions, careful patient selection using blood biomarkers. “There’s a huge amount of specialized knowledge in doing these studies right.”
Big Pharma’s Split Personality
After countless partnership discussions, Gourlay describes a peculiar dynamic: “The scientists know that non-amyloid targets are the way to go. But the marketing departments are very much like ‘you will talk about nothing but how good amyloid is.’ So there is a natural schizophrenia in those organizations which is a little sad.”
His explanation for why deals favor proven-but-marginal drugs over novel mechanisms: “If you think about the way business development works, it’s safe to go with something that’s proven, even if it’s only modestly effective. It’s a lot less safe to go with something new that may have a much bigger upside until it’s proven out.”
What’s Next
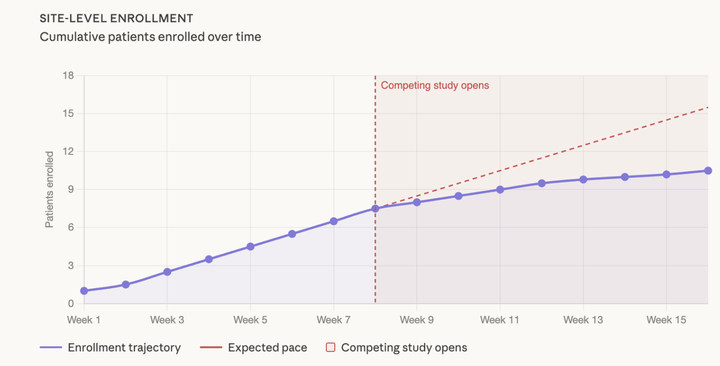
Phase 2b/3 trial enrolling now: 220 patients, 36 weeks, using blood biomarkers to select patients with active disease. Interim analysis roughly six months out, final results in late 2026. FDA consultations wrapped up with agreement on the approval pathway—one additional pivotal trial and limited extra studies needed.
The timeline matters. “This year is very much about regulatory consultations with the FDA,” Gourlay explains. The 100th patient should be enrolled in Q1 2026. Six months later, interim analysis confirms the trial isn’t futile. Then about a year after that, final results.
Gourlay flags one wildcard: GLP-1 receptor agonists (weight-loss drugs) showing lower Alzheimer’s rates in diabetic databases, with trials reading out late 2025. His take: “Even if those trials turn out to be positive, I don’t think they’ll necessarily be suitable for the majority of people with Alzheimer’s” given nausea and weight loss in patients who already forget to eat and are losing weight.
But the core opportunity remains clear. After tens of billions spent on amyloid with modest results, cortisol modulation offers a validated alternative with proven effects in depression and promising Alzheimer’s data. Once-daily pill. Clean safety profile. And a team that’s executed flawlessly before.
“We feel like we’re a long way down the path of clinical validation for cortisol,” Gourlay says. “A positive confirmatory study with final results in late 2026 will be a huge scientific discovery and confirmation of the cortisol hypothesis.”
Six months until interim data tells us if the pilot signal was real.
Comments ()