Your Best Sites Have Already Solved Your Patient Recruitment Problem
How "positive deviance" can help you find what's working and scale it
Many sponsors assume their sites are running similar recruitment processes. They’re often not.
Across a 50-site study, you may have 50 different approaches to that first patient phone screen. Different questions. Different order. Different objection handling. Different conversion rates.
The problem isn’t underperforming sites. It’s an “invisible variance.”
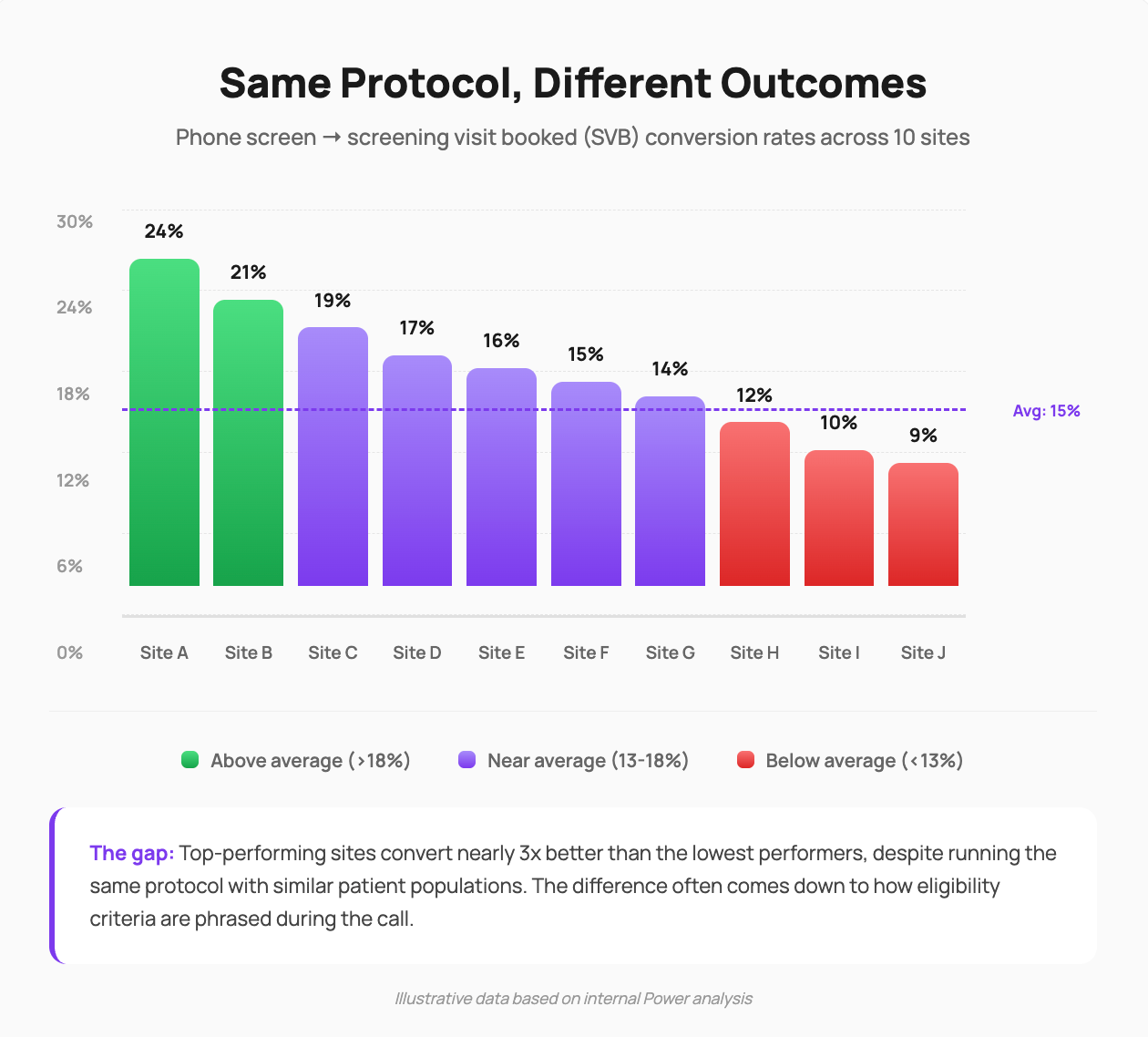
When Site A (as an example) converts 20% of phone screens and Site B converts 10%, sponsors typically attribute the gap to referral quality or patient demographics. Sometimes that’s accurate. Often, it’s the screening call itself.
But you can’t address what you can’t see.
A recent example from our network:
We ran this analysis for a recruitment program we’re supporting. Dozens of sites, same protocol, substantially different phone screen conversion rates.
When we investigated, we found something notable: just 2 criteria in the protocol were driving roughly 80% of the variance in outcomes across sites (internal Power analysis, Q4 2025).
Same questions on paper. Materially different ways of asking them.
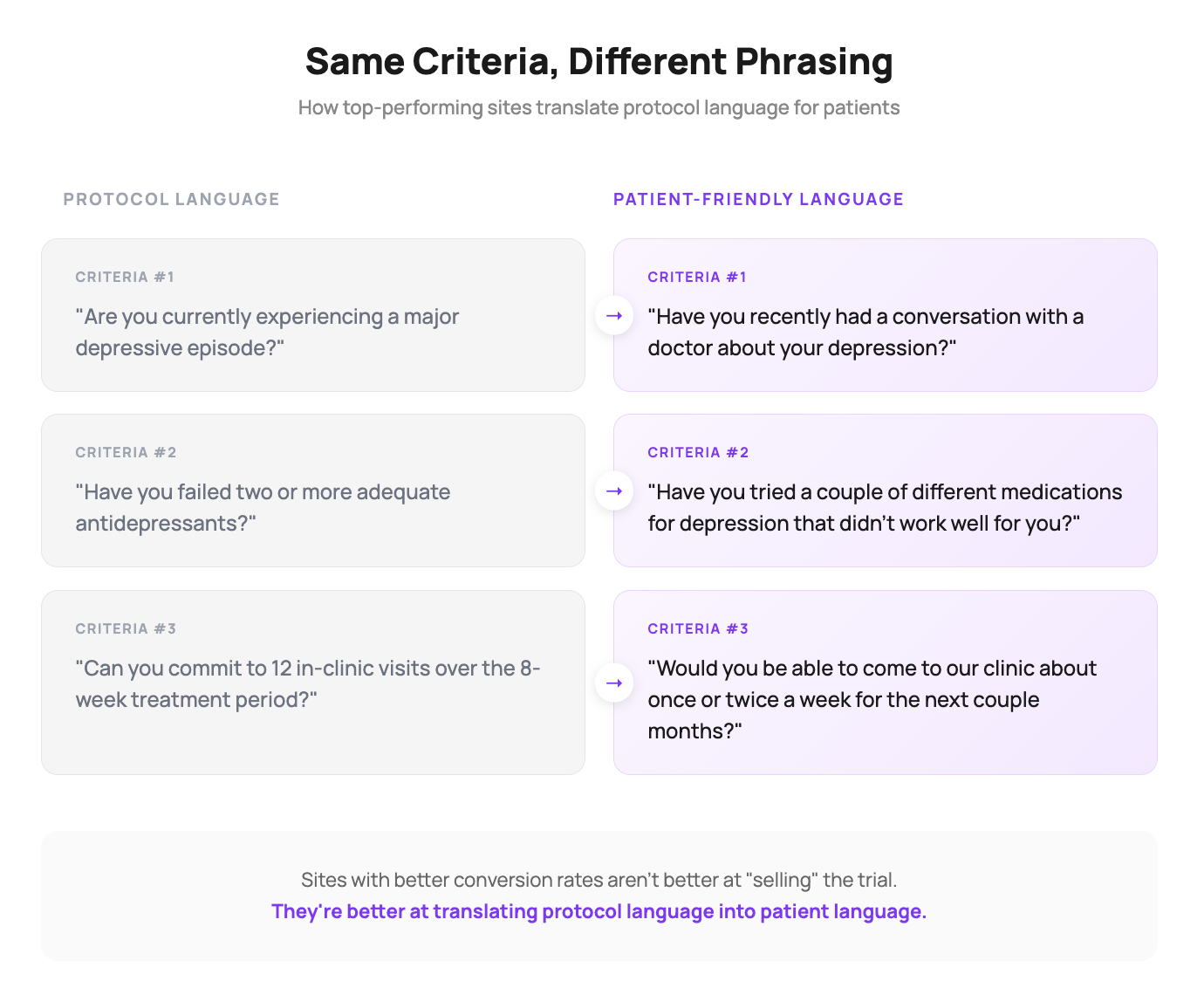
There are many ways to ask about the same medical history. And the way you ask matters considerably, because patients often struggle with clinical framing. One site asks “Are you currently experiencing a major depressive episode?” Another asks “Have you recently had a conversation with a doctor about your depression?” Same intent. Different patient response rates.
The sites with better conversion weren’t more effective at “selling” the trial. They were better at translating protocol language into patient language.
Harnessing positive variance
We call this approach “harnessing positive variance,” treating site-level differences not as noise to eliminate, but as signal to learn from.
I first learned this strategy at McKinsey, where we applied it across domains like retail store productivity and customer support operations. The underlying methodology is called “positive deviance,” rooted in public health research from the 1970s. The premise, as Richard Pascale put it in The Power of Positive Deviance (Harvard Business Press, 2010): “At least one person in a community, working with the same resources as everyone else, has already licked the problem that confounds others.”
The goal isn’t to import external best practices. It’s to find the positive deviants already in your network and scale what they’re doing.
See: Your Sites Are Losing Patients on Phone Screens (And You’d Never Know) for our earlier deep-dive on why phone screening represents a critical yet often-overlooked enrollment lever
Here’s how it works in practice:
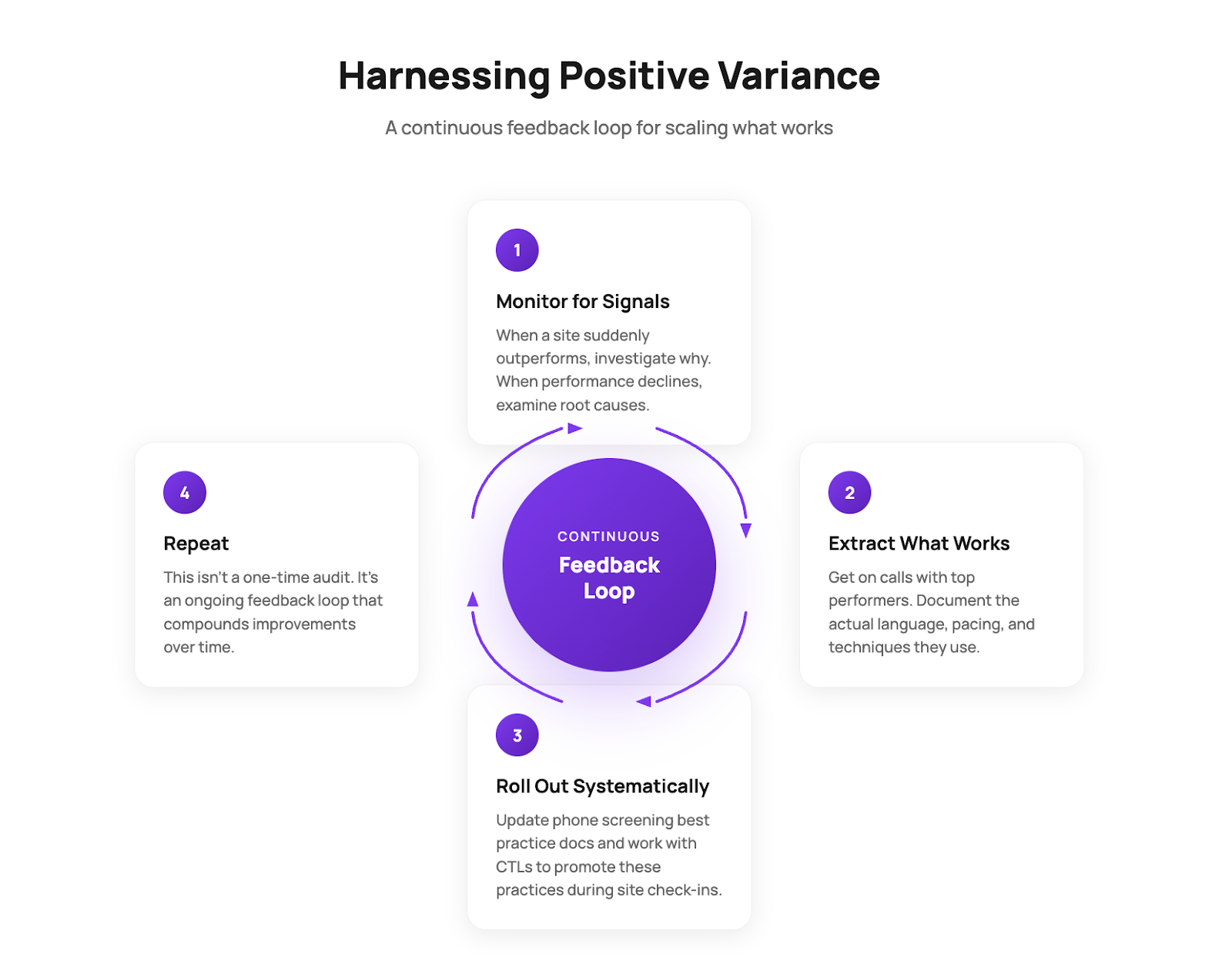
At Power, we run this loop continuously across programs we support, identifying positive variants, investigating root causes, and rolling out effective practices through our dedicated site account management team. Harnessing positive variance isn’t a one-time optimization. It’s integrated into how we work.
Also, if you haven’t already, read our 2025 Recap - What 10x Enrollment Growth Taught Us!
The compounding effect
A 5-point improvement in phone screen conversion across your network can translate to weeks or months saved on your enrollment timeline, without additional spending on patient acquisition. For context, our data across hundreds of sites shows median site performance at 52% of projected enrollment. Small gains at the phone screen stage compound through every downstream step of the funnel.
The sites that convert more effectively aren’t simply fortunate. They’re (often) doing something different on the phone.
The question isn’t whether variance exists in your network. It does. The question is whether you’re treating that variance as a problem to solve or an opportunity to learn from.
Your highest-performing sites have already figured something out. Your job is to find out what, and help everyone else do the same.
Comments ()