The Clinical Execution Playbook Behind Schizophrenia's First New Mechanism
How Karuna's former CMO turned disciplined trial methodology into a $14 billion BMS acquisition
When Steve Brannan joined Karuna Therapeutics in 2017 as employee number two, the company had a molecule shelved by Eli Lilly and not much else. Seven years later, Bristol Myers Squibb paid $14 billion for that molecule, now approved as Cobenfy, the first new mechanism for schizophrenia in over 50 years.

“We never skipped a beat. We never really had a stumble,” Brannan recalls. That track record came from methodological discipline applied consistently throughout development.
Note: do you have any questions about this article or how Power can help your clinical trial? You can book some time with us here.
The Xanomeline Revival Few Others Pursued
The science wasn’t new. Eli Lilly had shelved xanomeline years earlier after discovering it worked well for behavioral symptoms in Alzheimer’s patients, but the side effect burden made it unusable. The compound sat dormant until Karuna’s team asked a deceptively simple question: What if we block the peripheral side effects with an anticholinergic that can’t cross into the brain?
“Most of the benefits are central in your central nervous system and most of the side effects are peripheral,” Brannan explains. “Your central nervous system is protected. So not all things can get in there. So what if we block the peripheral side effects with an anticholinergic?”
The muscarinic agonist would hit M1/M4 receptors in the brain to reduce psychosis. Trospium would stay in the periphery to mitigate side effects. Simple in retrospect. Notable in execution.
When Brannan joined, Dr. Anantha Shekhar had already run a small 10-versus-10 schizophrenia trial that showed substantial effects. “It looked for all the world like this drug was really good at that,” Brannan says. The question wasn’t whether the mechanism worked... it was whether they could run trials precise enough to demonstrate it.
The Three Mistakes That Compromise CNS Trials
Brannan’s framework is blunt: “More is better. No, it’s not.”
Mistake 1: Too Many Sites Dilute Quality
“There’s probably a limited number of really high quality sites doing this kind of work in the US,” Brannan explains. “You go past the A sites into the B sites and then the C sites and then the D sites. You just add more variance.”
Karuna kept their site list tight. Brannan and Sharon Sachs, clinical operations lead from GSK, personally knew most principal investigators. “The sites working for us aren’t doing it because they know Karuna. They’re doing it because they know me and Sharon.”
That relationship capital mattered. “No one person knows everything and sees everything,” Brannan notes. Karuna solicited protocol feedback from sites before finalizing study designs.
Mistake 2: Speed Without Discipline
“I’ve been asked to make trials go faster many times. I’ve never been asked to slow one down.” The pressure to accelerate is constant. The discipline to resist is often tough.
His canonical example: at Takeda, the first wave of antidepressant trials went 0-for-8. Same compound, second wave went 4-for-5 positive. “One of the things was not getting in a hurry and doing stupid stuff.”
Before launching that second wave, Brannan made his team commit that they wouldn’t push for speed. “I’ll guarantee you one thing about this second wave of studies. They will not be as fast as the first time. Does everybody understand?”
Six months later, both Lundbeck and Takeda leadership were asking him to accelerate. “They can’t help themselves,” he says. “You need somebody that has the courage to sort of say no.”
Mistake 3: Ignoring the Data Stream
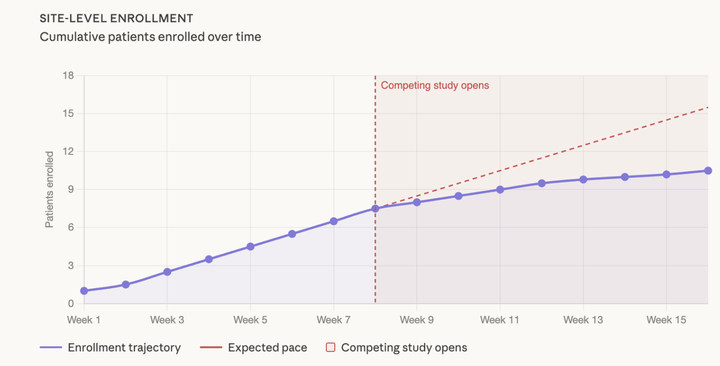
Karuna watched closely through blinded data analytics. When one site enrolled three consecutive patients over age 55, far above the trial’s median age of 42-44, Brannan called the PI directly.
“How long is the geriatric convention in town?” he asked. The PI understood immediately. He was funneling younger patients into a competitor’s trial that had a 55-year age cap, sending Karuna the overflow. “The next three patients they did were all under the age of 55.”
Gentle touch. Clear message. No antagonism. “You can’t be a mean bastard,” Brannan notes. “People don’t like working with you that way. But you can get your points across.”
What Actually Separated Karuna
Beyond site selection and pacing, Karuna implemented granular quality controls. Real-time rater monitoring tracked when site and central assessors diverged by more than a couple points on PANSS scores... immediate investigation followed. Protocol feedback loops with sites before finalization prevented operational burden. Direct sponsor engagement without hiding behind CROs built trust.
“Talk to me anytime, day or night,” Brannan told investigators. At CNS Summit and other conferences, he brought his clin ops team to meet sites face-to-face. When BMS attended one of these meetings post-acquisition, watching sites sing Brannan a farewell song over dessert, a BMS executive turned to him: “They really like you.”
Brannan’s response: “There’s three other trials out there competing for the same time and space.”
The Variance Problem Often Overlooked
“A lot of our endpoints are soft,” Brannan explains. “Depression... are you feeling less depressed today? It’s not a very hard solid thing. It fluctuates during the day.”
Unlike hemoglobin A1C in diabetes or tumor measurements in oncology, psychiatric outcomes require navigating inherent variance. The goal is to avoid adding to it through poor methodology.
Karuna’s PANSS mean of 97 with normal distribution across sites demonstrated that discipline. When variance appears where it shouldn’t, like three consecutive elderly patients at a single site, it signals noise creeping in. EMERGENT-3 showed an 8.4-point PANSS reduction versus placebo (p<0.0001) with methodology tight enough to detect the treatment effect.
The Lesson Investors Often Miss
At a major investor meeting in Boston, Brannan asked whether anyone evaluated clinical operations teams when assessing companies. “They’re like, ‘No, why would we do that?’ I’m like, ‘Because the execution of the trial is one of the major differences of whether you succeed or not, at least in CNS.’”
They nodded politely and moved on to discuss molecule mechanisms, market size, and competitive landscape. The clinical operations teams seemingly received little consideration in their investment calculus.
Three years later, that execution discipline contributed to a $14 billion valuation.
The broader lesson extends beyond Karuna. “Clinical trial methodology is the key to really having consistently good trials,” Brannan reflects. Yet the field often repeats the same mistakes: expanding beyond quality sites to hit enrollment targets, accelerating timelines under pressure, failing to monitor data streams for early warning signs.
Brannan’s career, spanning Cymbalta at Eli Lilly, work at Novartis and Takeda, and Forum Pharmaceuticals before Karuna, taught him what separates signal from noise in CNS trials. At Karuna, he finally had the authority to apply it comprehensively. “We had a lot of experience. We strategically knew the whole pathway from early to late,” he says. “We knew the right sites. We knew some of the CROs. A lot of the sites that were available knew who I was.”
That network, combined with “something really cool” scientifically, created favorable alignment. High-quality vendors like Signant and Syneos provided resources small companies don’t always receive “partly because they knew who I was and my track record as well as Sharon.”
For clinical operations directors wondering what made the difference: Karuna didn’t discover new methodology. They simply refused to compromise on fundamentals everyone knows but few execute consistently. Site quality over quantity. Optimal pacing over speed. Continuous data monitoring over assumptions. Collaborative relationships over transactional ones.
“I follow a fairly strict scientific method when it comes to clinical trials,” Brannan says. “I think clinical research should be as disciplined as any laboratory research.”
The approval demonstrates that in CNS trials, execution methodology can meaningfully influence trial outcomes. For clinical operations teams, the Karuna story offers a clear takeaway: methodological discipline, applied consistently from site selection through data monitoring, matters.
Related: The Alzheimer’s Hypothesis Big Pharma Missed - Another story of scientific discipline over conventional wisdom
Other: Interested in learning more about Power, book some time with us here!
Comments ()